Stay updated with the latest - Click here to follow us on Instagram
Journalism of Courage
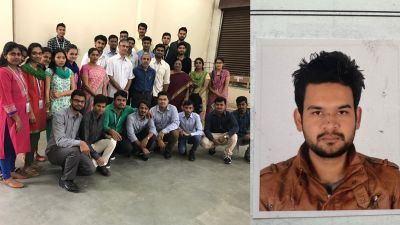
 Sneha Gond at Sewri TB hospital. TB is the sixth most common cause of death among women. Express
Sneha Gond at Sewri TB hospital. TB is the sixth most common cause of death among women. Express
ON Bed Number 348 of the Group of TB (GTB) Hospital in Sewri in central Mumbai, by the third week of August, a malnourished Sneha Gond, 22, could not move without help. Previously, she had been ready for discharge after three months in hospital, but there was nobody to take her home. Though she has an uncle, a younger brother and a sister in Chembur, for four years now, her home had been Niramay Niketan in Trombay, a shelter home for HIV-positive and tuberculosis patients.
“My uncle asked me to leave after I was diagnosed with HIV and TB. I was only 18,” she told The Indian Express. After her mother died in 2009 and her father left the family, the siblings lived with their uncle.
On September 6, when The Indian Express visited Sneha again in hospital, she had shrunk some more and required an adult diaper. “She says she wants to kill herself,” Shehnaaz Bano, another patient, said darkly. Sneha had cried herself to sleep. An on-duty nurse said she was showing signs of depression and suicidal tendencies. “We have asked for psychiatric counselling,” said the on-duty doctor.
Since 2013, five women patients have committed suicide at GTB Hospital. On September 9, Sneha Gond died. Doctors claim she died naturally, her immunity critically damaged. But Shehnaaz Bano, the patient who occupied the cot opposite Sneha’s for three months, believes otherwise. “Sneha had stopped eating food. No doctor or nurse will acknowledge it, but this was a suicide.”
Also Read Part I: Treated but abandoned, women with history of mental illness languish in institutions
Sneha’s is not a very unusual story among TB patients. While there are social support groups for women with HIV and cancer, there are none for those with tuberculosis, which accounts for more deaths than the other two.
“The government can provide treatment and counselling. But we need organisations to step forward and help those who suffer from TB and have no family support,” says Dr Padmaja Keskar, executive health officer of the Brihanmumbai Municipal Corporation (BMC) under which the GTB Hospital functions.
The hospital regularly refers to the local police station cases where patients have been abandoned for more than one year, but the latter, overburdened and stretched thin already, cannot trace every family. “Usually, such patients remain in the hospital until they die,” says a medical officer.
Dr Soumya Swaminathan, director of the Indian Council of Medical Research, says the Revised National Tuberculosis Control Programme (RNTCP) is still to incorporate within policy the concept of palliative support and rehabilitation for abandoned TB patients.
According to Stobdan Kalon, medical coordinator for Medecins Sans Frontierers (MSF), New Delhi, developing countries see a huge gap in palliative support to those who have failed TB treatment. “In Armenia, NGOs have come forward to provide social support. In Mumbai, we are training our volunteers at Tata Memorial Centre on palliative care for end-of-life-care for TB patients. But the burden of TB is so huge in India, it seems difficult to provide support to those who have finished treatment but have no family,” he said.
According to estimates, TB infects 32 lakh and kills over 10 lakh women globally every year. The disease is responsible for more deaths among women in the reproductive age group than all other causes of maternal mortality combined. In India, TB is the sixth most common cause of death among women. And the RNTCP-2017 report shows an incidence of 28 lakh TB cases, of which men report 2.25 times higher incidence than women, pegging the TB incidence among Indian women currently at 8.6 lakh.
Also Read Part II – Cancer: Hair loss, disfigurement, abandonment take toll on women
“Our stories are all the same,” says Aisha Siddiqui, 20, hospitalised for the past two months with pulmonary TB. Frail women around her bed in GTB Hospital nod weakly. Siddiqui got married in 2015, but her husband has not visited her in hospital even once. She speaks to him over the phone once every few days, urging him to come visit. “I take 14 medicines daily. They burn my body,” says the Mumbra resident. Aisha’s mother commutes 50 km every day to meet her. “Gareebi me beemari me kaun kiska hota hai (There is no one for the poor who take ill),” Aisha rues.
Extrapulmonary TB in the lymph nodes is a common TB among women. Adherence to treatment is higher among women, so women are less likely to die, default or fail treatment. But diagnosis itself may be a problem for them.
A study by the National Center for Biotechnology Information (NCBI) points towards possible under-reporting of TB among Indian women. “Gender differentials exist in reporting and diagnosing TB, and passive case finding likely leads to failure to diagnose TB in women,” says the report, citing socioeconomic and cultural factors and difficulty for women to access healthcare.
Shalini Bharat, professor at the Tata Institute of Social Sciences, says the country needs an articulate policy that recognises there is gender-based disparity in healthcare for TB patients. “And then we must create programmes that directly deal with these issues,” says Bharat. Her field project Saksham, which counsels TB patients and their family members on the importance of TB treatment in Karnataka, Maharashtra, Rajasthan and Gujarat, found that adherence to treatment is better in families where there is counselling and lower stigma.
Shashikala Shinde, social worker at Niramay Niketan, agrees that such patients need skill training and educational support. “Families should not abandon them,” she says. Sneha Gond, one of her inmates at Niramay, had tried repeatedly to reach out to her brother and two sisters for moral support, she says. Sneha had wanted to work after recovery. Eventually, the GTB Hospital managed to bring Sneha’s family, including her father who had abandoned her, for a visit. Records show they met her briefly in September, but flatly refused to take her home. She was subsequently put on psychiatric medication, but eventually died after days of not eating anything.
A nurse who has looked after TB patients for 12 years says a husband’s or family member’s support is crucial for recovery of women patients. She cites Yamuna Nande, 70, as an example. The septuagenarian has been in GTB Hospital for seven months after her neighbours in Trombay brought her. “I have a brother, a niece in Bandra. But they haven’t come to hospital,” Nande says. She has a poly bag with some clothes, everything she owns. “Will you help me? I don’t want to die here.”
Stay updated with the latest - Click here to follow us on Instagram
You May Like