© The Indian Express Pvt Ltd
Premium
This is an archive article published on June 12, 2023
Testing to prevent heart attack in asymptomatic people: Required, wasteful or dangerous?
These tests are not 100 per cent accurate and a positive result does not always mean the individual has the disease. And vice versa. Such tests in asymptomatic individuals are generally not recommended and might even be dangerous, says Tushar Gore
Written by Tushar Gore
Updated: June 21, 2023 09:30 AM IST
 The Treadmill Test (TMT) is done to determine the health of the heart. (Source: Getty Images)
The Treadmill Test (TMT) is done to determine the health of the heart. (Source: Getty Images)
Listen to this article
Testing to prevent heart attack in asymptomatic people: Required, wasteful or dangerous?
x
00:00
Cardiac health first shows up on the radar as a concern in the middle age, even in asymptomatic individuals. It perhaps reaches the top of mind for short durations upon hearing of someone’s collapse due to a surprise heart attack. In the face of uncertainty, many individuals might think of tests – the most common one is the Treadmill test (TMT) – as a way to alleviate the anxiety about having a surprise heart attack.
There is abundant information regarding tests for detecting cardiovascular (CV) disease. A crucial knowledge gap, however, is the accuracy of these tests. These tests are not 100 per cent accurate and a positive result does not always mean the individual has the disease. And vice versa. Such tests in asymptomatic individuals are generally not recommended and might even be dangerous.
NO TEST IS 100 PER CENT ACCURATE
Similar to any measurement, diagnostic tests have a margin of error and yield false results. A false positive is a positive result (i.e., presence of disease) that is incorrect. That means the test incorrectly labels a healthy person as diseased. Similarly, a false negative incorrectly marks a diseased person as healthy. Any test has to accomplish two goals: correctly identify the diseased and the healthy individuals. The two goals are distinct and one can be achieved without the other.
To illustrate the point, let’s consider this extreme example: Imagine a test that labels everyone as diseased. This test would work remarkably well if a large majority of the individuals tested with it were actually sick but it would fail miserably if most of them were healthy people. Thus, it would correctly identify the diseased people, but fail to find the healthy ones. Therefore, accuracy of a test is measured by two parameters – aligned with the two goals. Sensitivity is the ability of the test to correctly identify diseased individuals. A highly sensitive test picks up a large percentage of the diseased. It is calculated as the number of positives detected out of the number of diseased individuals tested.
A test with 90 per cent sensitivity will correctly identify nine individuals out of the 10 sick individuals that take the test.
The second measure – the ability to correctly identify healthy individuals – is called specificity. It is calculated in a similar manner. Sensitivity and specificity are independent of each other.
DO I BELIEVE MY TEST RESULT?
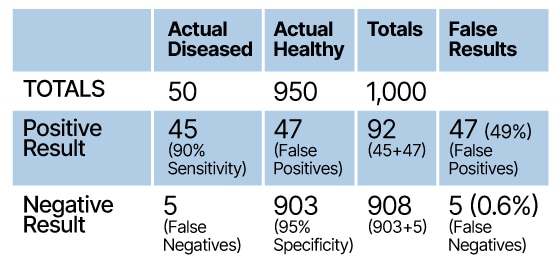
Let us imagine a test with 90 per cent sensitivity and 95 per cent specificity. Suppose the test is conducted in a population with five per cent disease prevalence (five per cent of the population has the disease). The disease prevalence is an important parameter. The true spread of the disease is, however, not always known and typically an estimate is used for prevalence. Let us test 1,000 people from this group. Our assumptions indicate that 50 have the condition (five per cent disease prevalence) and 950 are healthy. The table below shows the actual test results for these 1,000.
Story continues below this ad
 (Designed by Abhishek Mitra
(Designed by Abhishek Mitra
Out of the 50 diseased people, this test correctly identifies 45 and marks five as negative. And among the 950 healthy people, 903 (95 per cent) are correctly identified, and 47 are wrongly labelled with the disease.
Although the actual number of diseased people is only 50, this test marks 92 individuals (45 actual, plus 47 false positives). Since only 45 out of the 92 positive results (49 per cent) are actually sick, a person who receives a positive result will only be 49 per cent likely to have the disease. This ratio is called the positive predictive value, or post-test probability of disease, and indicates the degree to which a positive test can predict actual sickness. It should be as high as possible to drive confidence in a positive result.
Similarly, there is a negative predictive value and it indicates confidence in a negative result. In this example, a negative result has a 99.4 per cent probability of being accurate (903 out of 908 negative results are actually healthy). One insightful way to interpret these results is to compare the probability of being sick before and after the test. Before the test is taken, the probability of a person being sick (called pre-test disease probability) is five per cent – same as the disease prevalence.
A positive test increases this probability to 49 per cent (post-test disease probability). Interestingly, the probability of being healthy also increases with this test. Before the test, the probability of being healthy is 95 per cent. A negative result increases this probability to 99.4 per cent.
Story continues below this ad
So, this test increases the confidence in either diagnosis. A good test is one that raises this confidence to very high levels.
REDUCING FALSE RESULTS
In this scenario, the high number of false positives, 47, was a result of 95 per cent specificity and 950 healthy individuals. In most contexts, 95 per cent accuracy would be considered good enough. But in a situation with low disease prevalence, a test of much higher specificity is required. To push the false positives down to, let’s say, 10, a test with 99 per cent specificity is needed (based on above calculations with 99 per cent specificity).
Increasing specificity is one way to reduce false positives. The math indicates that another way is to increase the relative number of individuals with the disease. In the real world, this is achieved by testing in a population in which the disease is more widespread. That is, by limiting testing to a sub-group that is more likely to have the disease – as example, to people with CV disease symptoms or with multiple CV risk factors.
Repeating the above calculations with a population size of 500 with 50 diseased people (10 per cent prevalence) reveals that false positives come down to 22. The positive predictive value (confidence in a positive result) increases from 49 per cent to 67 per cent.
Story continues below this ad
In summary, false positives are reduced with two levers: a high specificity test, and a high disease prevalence setting (high pre-test disease probability).
Similar logic indicates that false negatives are reduced with a high sensitivity test used in a situation with low disease prevalence.
IMPLICATIONS FOR CARDIOVASCULAR DISEASES
There are many CVD tests. The goal of these tests is to determine whether the individual has “blockages” in the coronary arteries. These tests should be used in the correct settings. Otherwise depending upon the test’s accuracy, the results could be meaningless.
As an example, the most common test, the Treadmill Test (TMT) – also known as the Exercise Stress Test – has low sensitivity and specificity values of about 75 percent.
Story continues below this ad
Thus, testing in asymptomatic individuals – as is done in annual health checks – is an entirely incorrect use of this test.
One estimate of prevalence of clinical CVD (disease with some symptoms) in the overall population is 10 percent. Running the calculation in the table above with these numbers gives a Positive Predictive Value for the stress test of 25 per cent! So, a positive test result can hardly be believed. In the real world, however, a positive result leads to further invasive testing to confirm or rule out the disease. This subsequent invasive testing is one of the main risks of the stress test (or of any inaccurate test). Similar evaluations should be conducted for other tests as well.
CV disease is an extremely complex disease and the causes of a surprise heart attack are multi-fold. Presence of blockages is only one (albeit critical) element. An explainer on blockages and heart attacks, explains the mechanism of a surprise heart attack. Many occur in individuals having “small” blockages – blockages that do not cause symptoms, and are therefore undetectable by tests such as the TMT. Hence, such testing in asymptomatic individuals should be avoided. The American Heart Association (AHA) has detailed guidelines that assess risks of heart attack in asymptomatic population, and these guidelines refrain from recommending tests other than routine blood tests – except in a narrowly defined group.
(Dr Tushar Gore is the managing director of Resonance Laboratories, a niche pharmaceutical manufacturer. He studied at IIT-Bombay and the University of Minnesota, and has worked at McKinsey and Novo Nordisk. His focus area is pharmaceuticals)
Advertisement

Live Blog
Photos





Top Stories











Advertisement
Must Read







Advertisement
Buzzing Now
TrendingTinder scam: Delhi man claims Karkardooma cafe trapped him with Rs 50,000 bill on first date

TrendingCanadian woman claims she was denied apartment in Toronto since she's not Gujarati: ‘This is sad and pathetic’

Trending‘Haters ko fan banane ka ghamand’: GST rate cut memes take over the Internet, see the best ones here



- 01
- 02
- 03
- 04
- 05
Advertisement