© The Indian Express Pvt Ltd

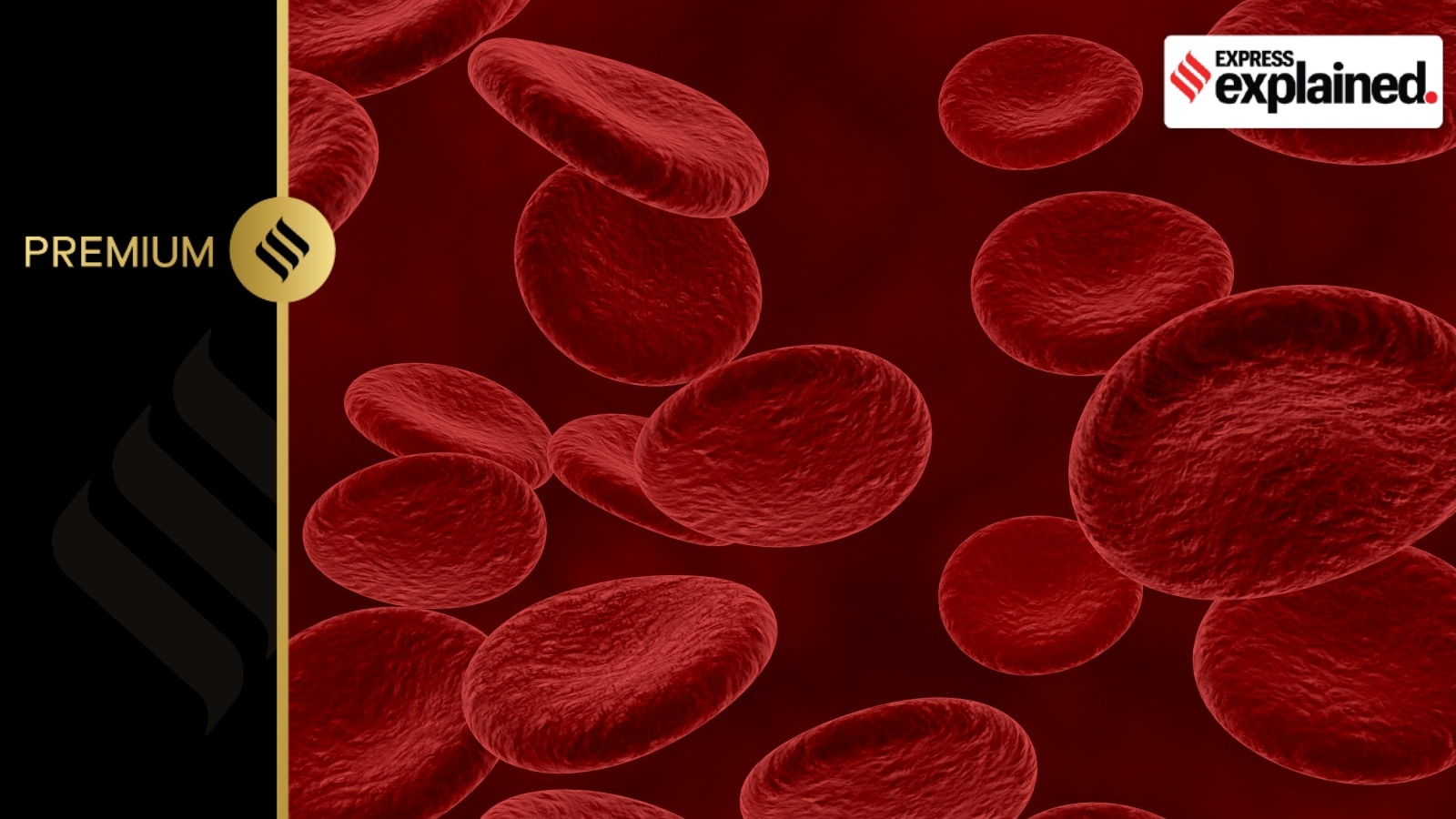 The genetic error in sickle cell disease leads to red blood cells (seen here normally) assuming a crescent shape. These cells cannot move around easily in the vessels as a result, leading to blocked blood flow. (Photo via Freepik)
The genetic error in sickle cell disease leads to red blood cells (seen here normally) assuming a crescent shape. These cells cannot move around easily in the vessels as a result, leading to blocked blood flow. (Photo via Freepik) The UK drug regulator last week approved a gene therapy for the cure of sickle cell disease and thalassaemia, seen as a landmark breakthrough by many. This is the first licensed therapy in the world based on the gene editing technology Crispr-Cas9 that earned its innovators a Nobel Prize in 2020.
The “genetic scissors” that became available for the first time in 2012 have revolutionised the field of biotechnology.
Called Casgevy, the therapy edits the faulty gene that leads to these blood disorders, potentially curing the person for life. So far, the only permanent treatment has been a bone marrow transplant, for which a closely matched donor is needed.
Both sickle cell disease and thalassaemia are caused by errors in the gene for haemoglobin, a protein in the red blood cells that carry oxygen to organs and tissues.
The therapy uses the patient’s own blood stem cells, which are precisely edited using Crispr-Cas9. A gene called BCL11A, which is crucial for switching from foetal to adult haemoglobin, is targeted by the therapy.
 How sickle cell disease works.
How sickle cell disease works.
Foetal haemoglobin, which is naturally present in everyone at birth, does not carry the same abnormalities as adult haemoglobin. The therapy uses the body’s own mechanisms to start producing more of this foetal haemoglobin, alleviating the symptoms of the two conditions.
The genetic error in sickle cell disease leads to red blood cells assuming a crescent shape. (See graphic above) Unlike the disc shaped normal cells, the sickle-like cells cannot move around easily in the vessels, resulting in blocked blood flow. This can lead to episodes of severe pain, life-threatening infections, anaemia, or a stroke.
An estimated 30,000-40,000 children in India are born with the disorder every year.
The symptoms manifest in people who inherit a pair of damaged genes from both parents. Those who carry only one copy of the gene from one parent can lead a normal life. This is the same as thalassaemia, in which people who inherit a pair of genes from both parents experience symptoms like severe anaemia.
Thalassaemia leads to low levels of haemoglobin, leading to fatigue, shortness of breath, and irregular heartbeats. People with the condition need blood transfusions throughout their life. The transfusions also lead to accumulation of excess iron in the body, for which they need chelation.
India also has the largest number of children with thalassaemia major in the world — about 1-1.5 lakh.
For sickle cell disease, 45 people received Casgevy. Only 29 of these patients had been in the trial long enough for the interim analysis on which the approval is based. All but one of these 29 trial participants had no severe pain crises for at least 12 months after treatment.
The therapy has been administered to 54 persons with thalassaemia for the trial. Of them, 42 were in the trial long enough for the interim analysis. 39 of the 42 patients did not need a transfusion for at least 12 months after the treatment. The need for transfusion dropped by 70% in the other three.
Casgevy is a one-time treatment for which the doctor has to first collect blood stem cells from the bone marrow using a process called apheresis — used to filter out the blood for different components. The cells are then sent to the manufacturing site where it takes about six months for them to be edited and tested.
Before a transplant with the edited cells, the doctor gives a conditioning medicine for a few days to clear the bone marrow of other cells that will be replaced by the modified cells.
The patient has to stay in hospital for at least a month so that the edited cells take up residence in the bone marrow and start making red blood cells with normal haemoglobin.
Side effects from the treatment are similar to those associated with autologous stem cell transplants, including nausea, fatigue, fever and increased risk of infection.
Although the price of the therapy hasn’t been announced, it is likely to be very high. Estimates suggest it could be as much as $2 million per patient, which is in line with other gene therapies. Cost is one of the biggest limitations of newer gene therapies, along with the absence of local manufacturing facilities, which means that the harvested blood stem cells have to be sent across countries.
“This is extremely encouraging as this is the first Crispr-based therapy that has been approved. But the pricing will be a major challenge, especially because a high proportion of people with these conditions live in poorer countries and are unlikely to be able to afford the therapy,” Dr Debojyoti Chakraborty from CSIR Institute of Genomics and Integrative Biology (CSIR-IGIB) said.
However, “The prices will likely come down as more and more people work on it,” he said. “Developing local manufacturing facilities will also help.”
Dr Chakraborty’s team is also working on a gene therapy for sickle cell disease with the government’s big push. The team is currently working on the pre-clinical studies and are likely to enter clinical trial in the next few years.